In Nephsap review we learned that cancer following cytoxan carries risk due to total dosing amount
low dose of cytoxan usually means < 36gm of total cumulative cytoxan exposure
( this is artbitary)
<36gm group most common cancers were non melenoma skin and basal cell cancers
>36gm group most common cancers were non melenoma skin and basal cell but also saw bladder cancers, AML( which happened after many years)

Thursday, September 30, 2010
Nephsap review: Glomerular, vascular and TI disease
In reviewing IgA Nephropathy:
Did you know that besides the pathology related prognostic signs, non traditional factors such as obesity, elevated nocturnal BP and increased uric acid levels and increased C4d mesangial depostion have been associated with a poorer prognosis in igA Nephropathy. A mild alcohol consumption and mild elevation in bilirubin with a improved outcome.
Interesting ! Likely due to anti oxidant effects of both
Did you know that besides the pathology related prognostic signs, non traditional factors such as obesity, elevated nocturnal BP and increased uric acid levels and increased C4d mesangial depostion have been associated with a poorer prognosis in igA Nephropathy. A mild alcohol consumption and mild elevation in bilirubin with a improved outcome.
Interesting ! Likely due to anti oxidant effects of both
Wednesday, September 29, 2010
Transplant Glomerulopathy
Transplant Glomerulopathy(TG) is a common biopsy finding that we see in kidney biopsies for proteinuria workup.The causes of TG are usually of similar to what causes secondary MPGN. Most of the time it turns out to be chronic antibody mediated rejection process. Pathologically, it is defined by glomerular basement membrane duplication with peritubular capillary basement membrane multilayering (PTCML), and associated with anti-human leukocyte antigen antibodies and C4d.
A recent study in Transplantation 2010 issue talks about possible predictors of long term outcomes of pure TG cases. 36 cases were noted. Only 33% were c4D positive. but the C4d-positive cases also showed a trend toward rapid graft loss. Interstitial fibrosis, PTCML, and arteriolar hyalinosis were significant predictors of graft survival in TG. C4d positivity was associated with a more rapid rate of function decline. eGFR slope data showed significant deterioration in graft function well before the diagnostic biopsy.
References:
http://www.ncbi.nlm.nih.gov/pubmed/20838279
http://www.ncbi.nlm.nih.gov/pubmed/19594595
A recent study in Transplantation 2010 issue talks about possible predictors of long term outcomes of pure TG cases. 36 cases were noted. Only 33% were c4D positive. but the C4d-positive cases also showed a trend toward rapid graft loss. Interstitial fibrosis, PTCML, and arteriolar hyalinosis were significant predictors of graft survival in TG. C4d positivity was associated with a more rapid rate of function decline. eGFR slope data showed significant deterioration in graft function well before the diagnostic biopsy.
References:
http://www.ncbi.nlm.nih.gov/pubmed/20838279
http://www.ncbi.nlm.nih.gov/pubmed/19594595
TOPIC DISCUSSION: Proximal Tubular Dysfunction
A nice discussion was done yesterday on Proximal Tubular function and then dysfunction.
A nice way that describes' the breakdown of these disorders : As suggested by Dr.A Bellucci.
Proximal Dysfunction can be:
1.Hemodynamically mediated
2.Altered Membrane Transport
3.Altered Intracellular Processes
So lets take them one by one.
1. Volume expansion decreases proximal tubular reabsorption (higher pcP and lower pcP): met acidosis (bicarbonaturia) & low BUN and leading to a physiologic prox tubular dysfunction. A pathologic example of this is renal vein thrombosis
2. Altered membrane transports are the ones that specifically lead to either bicarbonaturias or phosphaturias. Examples of these are: Osteopetrosis, Carbonic anhydrase inhibitor use, tumor induced osteomalacia or too much FGF 23
3. The last one is the ones we always encounter:- Myeloma, Ifosphomide toxicity, Heavy metal toxicity and in children: cystinosis, Dent's Diseases and Lowe's disease.
A nice way that describes' the breakdown of these disorders : As suggested by Dr.A Bellucci.
Proximal Dysfunction can be:
1.Hemodynamically mediated
2.Altered Membrane Transport
3.Altered Intracellular Processes
So lets take them one by one.
1. Volume expansion decreases proximal tubular reabsorption (higher pcP and lower pcP): met acidosis (bicarbonaturia) & low BUN and leading to a physiologic prox tubular dysfunction. A pathologic example of this is renal vein thrombosis
2. Altered membrane transports are the ones that specifically lead to either bicarbonaturias or phosphaturias. Examples of these are: Osteopetrosis, Carbonic anhydrase inhibitor use, tumor induced osteomalacia or too much FGF 23
3. The last one is the ones we always encounter:- Myeloma, Ifosphomide toxicity, Heavy metal toxicity and in children: cystinosis, Dent's Diseases and Lowe's disease.
TOPIC DISCUSSION: FENA less than one causes!
“Crrap 'n' cheap”
•Cardio-renal syndrome
• Renal Artery Stenosis
• Renal allograft rejection
• Acute interstitial nephritis
• Pre renal
• Non-oliguric ATN
• Contrast nephropathy
• Hepato-renal syndrome
• Early obstructive disease
• Acute Glomerulonephritis
• Pigment nephropathy
Although the test was designed originally in Oliguric patients. So how much use we have of it. Who knows! but above list is usually where we see FeNa<1
Tuesday, September 28, 2010
IN THE NEWS- Intestinal Dialysis

You can check it out at the following website.
http://today.uchc.edu/features/2010/may10/whale.html
We think of mostly three modalities when it comes to Renal Replacement Therapy( HD, PD and Transplantation). In some countries, they still use an another option as mentioned above. Intestinal dialysis, the patient is given soluble fibers such as mannitol, charcoal, acacia gum which then leads to increased nitrogenous fecal wasting leading to decreasing BUN and Crt. One study in Argentina studied the combination of a low protein diet and oral activated charcoal to reduce serum urea and creatinine levels in very old ESRD patients who had refused to start chronic dialysis. Nine lucid, very old > 80 years, ESRD patients who had refused to start dialysis were prescribed a treatment based on a combination of a very low protein diet and oral activated charcoal (30 gram/day). None of the patients had anuria, oliguria, edema, significant metabolic acidosis or hyperkalemia. None of them had significant gastrointestinal symptoms. After one week and ten months of charcoal use signi ficant decrease in blood urea and creatinine levels was observed.
Interesting that we don't offer this to someone with potential not wanting dialysis as a resort.
This should be looked into further.
Take a look at these references:
http://www.ncbi.nlm.nih.gov/pubmed/20061701
http://biomed.uninet.edu/2008/n1/musso-carta-en.html
Image source: Allrefer.com
Monday, September 27, 2010
IN THE NEWS- HUS review
The most recent issue of Seminars in Thrombosis and Homestatis has dedicated the entire journal to articles on HUS and atypical HUS. The reviews start with the old HUS definitions and then introduced atypical HUS syndromes and treatments and the most important of all- the role of complement pathway in this sequence.
Look below to see all the articles in the series.
http://www.ncbi.nlm.nih.gov/pubmed
("Semin Thromb Hemost"[Journal] OR "seminars in thrombosis and hemostasis"[All Fields]) AND HUS[All Fields] AND 2010[All Fields]
http://www.ncbi.nlm.nih.gov/pubmed/20865637
http://www.ncbi.nlm.nih.gov/pubmed/20865640
Look below to see all the articles in the series.
http://www.ncbi.nlm.nih.gov/pubmed
("Semin Thromb Hemost"[Journal] OR "seminars in thrombosis and hemostasis"[All Fields]) AND HUS[All Fields] AND 2010[All Fields]
http://www.ncbi.nlm.nih.gov/pubmed/20865637
http://www.ncbi.nlm.nih.gov/pubmed/20865640
Sunday, September 26, 2010
IN THE NEWS- Low Magnesium = Diabetes Risk
A recent study done with at UNC of 5000 patients showed that with increase in Magnesium intake, the risk of diabetes decreased. Take a look at the recent Post of Uremic Frost and also the study listed below.
In the basic science world, there always has been some speculation about magnesium deficiency and insulin resisntance and we also recently showed that post transplant hypomagnesemia was an independent risk factor of new onset Diabetes.
It is all falling into place!
Also see
http://www.uremicfrost.com/2010/09/magnesium-may-decrease-risk-of.html
http://www.ncbi.nlm.nih.gov/pubmed/20807870
http://www.renalandurologynews.com/new-onset-diabetes-linked-to-post-transplant-hypomagnesemia/article/169297/
In the basic science world, there always has been some speculation about magnesium deficiency and insulin resisntance and we also recently showed that post transplant hypomagnesemia was an independent risk factor of new onset Diabetes.
It is all falling into place!
Also see
http://www.uremicfrost.com/2010/09/magnesium-may-decrease-risk-of.html
http://www.ncbi.nlm.nih.gov/pubmed/20807870
http://www.renalandurologynews.com/new-onset-diabetes-linked-to-post-transplant-hypomagnesemia/article/169297/
Saturday, September 25, 2010
Friday, September 24, 2010
IN THE NEWS- " Its not me, its the guy next to me" , says MYH9
 Gene variants of MHY9 locus were being considered as possible risk factors for FSGS and high incidence of kidney diseases in the african american population for the last decade. A further risk assessment was just done by the same investigators and 1641 European Americans were compared to 1800 African Americans and new locus was discovered.
Gene variants of MHY9 locus were being considered as possible risk factors for FSGS and high incidence of kidney diseases in the african american population for the last decade. A further risk assessment was just done by the same investigators and 1641 European Americans were compared to 1800 African Americans and new locus was discovered.What is more interesting is why did this selection process happen?
A nice analogy is like Sickle Cell and Malaria- here the association seems to be Trypanosoma Brucei, parasite commonly found in Africa that causes sleeping sickness and FSGS. So having this mutation protects you against sleeping sickness but puts you at higher risk now of FSGS and glomerular diseases and more accelerated sclerosis.
A little something on Sleeping Sickness also called African Lethargy or Trypananosomiasis.

It is transmitted by the tsetse fly. The disease is endemic in some regions of sub-Saharan Africa, covering about 36 countries and 60 million people. It is estimated that 50,000 to 70,000 people are currently infected, the number having declined somewhat in recent years. Four major epidemics have occurred in recent history: one from 1896–1906 primarily in Uganda and the Congo Basin, two epidemics in 1920 and 1970 in several African countries, even a recent epidemic in 2008. The symptoms occur in two stages. The first stage is known as the haemolymphatic phase and is characterized by fever, headaches, and joint pains, and itching. If left untreated, the disease overcomes the host's defenses and can cause more extensive damage, broadening symptoms to include anemia and multi organ failure. The second stage, called the the sleeping phase and leads to more confusion and involvement of the CNS system leading to drowsiness and hence the disease's name. Apparently, this disease can be transmitted vertically and via sexual means as well!!
The link to APOL1 was first noted when a new treatment based on a truncated version of the apolipoprotein L-1 of HDL and a single domain antibody was found to work in mice. And now this organism's long history is causing kidney diseases due to what some might call "epi genetic phenomenon"
This is fascinating and exciting new theories. Lets see what more studies pan out.
References:
http://www.ncbi.nlm.nih.gov/pubmed/20668430
http://www.ncbi.nlm.nih.gov/pubmed/20647424
http://www.ncbi.nlm.nih.gov/pubmed/20688934
Thursday, September 23, 2010
CONSULT ROUNDS: Parvovirus b19 and transplant patients
 Parvovirus B19 is a common human pathogen, causing erythema infectiosum in children, hydrops fetalis and transient aplastic crisis in patients with chronic hemolytic anemia.
Parvovirus B19 is a common human pathogen, causing erythema infectiosum in children, hydrops fetalis and transient aplastic crisis in patients with chronic hemolytic anemia. Renal transplant recipients can develop symptomatic B19 infections as a result of primary infection acquired via the usual respiratory route or via the transplanted organ, or because of reactivation of latent or persistent viral infection. It is not something we commonly think about or screen for.
The most common manifestations of B19 infection in immunosuppressed patients are pure red cell aplasia and other cytopenias. If you have a patient with unexplained anemia, and the reticulocyte count is also low, think of Parvovirus B19 in the differential, get PCR. You shall be surprised how many you will pick up.
It can affect the kidney post transplant as well and can lead to a post Transplant Collapsing Glomerulopathy.(PTCG). Before it gets to that stage, treatment might be crucial. Thrombotic microangiopathy have been reported in association with B19 infection in renal transplant recipients, but a causal relationship has not been definitively established. Most patients benefit from intravenous immunoglobulin therapy and/or alteration or reduction of immunosuppressive therapy.
References:
http://www.ncbi.nlm.nih.gov/pubmed/20842928
http://www.ncbi.nlm.nih.gov/pubmed/17895931
http://www.ncbi.nlm.nih.gov/pubmed/19099488
CMV and EBV PCR for 2 years
Check out this interesting post from Dr.Sethi
https://www.pediatric-nephrology.com/home/2010/09/23/300-jasnviremia.html
https://www.pediatric-nephrology.com/home/2010/09/23/300-jasnviremia.html
B cells in Transplantation
Recently at the ATC 2010, a nice abstract was presented regarding Regulatory B cells. They are coming!!!
T cell immunglobulin and mucin -1 or TIM-1 is a costim molecule that controles T effector cells.
The listed abstract below showed that Tim-1 is more highly expressed on naive B cells than on T cells.
Depleting B cells led to Tim-1 accelerated islet cell rejection in these mice. Re constitution of B cells led to prolonged graft survival and and transfer of Tim-1 + B cells prolonged allograft survivial suggesting that Tim-1 + b cells could be B regulatory cells like Foxp3+ T reg cells.
Again, no human data yet. more studies to come!
Exciting stuff!
Reference:
Ding Q, Yueng M, Najafian N, et al. Regulatory B cells are identified by TIM-1 and can be induced through TIM-1 ligation to promote allograft survival. ATC 2010, San Diego, Calif, Abstract 167.
T cell immunglobulin and mucin -1 or TIM-1 is a costim molecule that controles T effector cells.
The listed abstract below showed that Tim-1 is more highly expressed on naive B cells than on T cells.
Depleting B cells led to Tim-1 accelerated islet cell rejection in these mice. Re constitution of B cells led to prolonged graft survival and and transfer of Tim-1 + B cells prolonged allograft survivial suggesting that Tim-1 + b cells could be B regulatory cells like Foxp3+ T reg cells.
Again, no human data yet. more studies to come!
Exciting stuff!
Reference:
Ding Q, Yueng M, Najafian N, et al. Regulatory B cells are identified by TIM-1 and can be induced through TIM-1 ligation to promote allograft survival. ATC 2010, San Diego, Calif, Abstract 167.
Infections post transplant
We had a good discussion about infections post transplant yesterday ranging from rare cases of Parvovirus B19 to common bacterial infections
A timeline is important to keep in mind.
<1Month into transplant
Think of the common post surgical fever causes
MRSA, Pneumonias
Wound infection
C.diff
Aspiration
BKV can be seen as early as 2 weeks( depending on net immunosuppression state of the patient)
1-6 months into transplant
BK Nephritis
Adenovirus
CMV, PCP
HCV
MAC
>6 months
Back to normal population infections
But also
Nocardia
Atypical fungi
West nile
JC virus( PML)
CMV can happen here as well
So can BKV
A nice review is listed below from NEJM
http://www.ncbi.nlm.nih.gov/pubmed/18094380
A timeline is important to keep in mind.
<1Month into transplant
Think of the common post surgical fever causes
MRSA, Pneumonias
Wound infection
C.diff
Aspiration
BKV can be seen as early as 2 weeks( depending on net immunosuppression state of the patient)
1-6 months into transplant
BK Nephritis
Adenovirus
CMV, PCP
HCV
MAC
>6 months
Back to normal population infections
But also
Nocardia
Atypical fungi
West nile
JC virus( PML)
CMV can happen here as well
So can BKV
A nice review is listed below from NEJM
http://www.ncbi.nlm.nih.gov/pubmed/18094380
Wednesday, September 22, 2010
Tuesday, September 21, 2010
Renal Fellow Network: Doc, I am very sensitized! (part 2)
Renal Fellow Network: Doc, I am very sensitized! (part 2): "Let’s continue our discussion from our last blog about sensitized kidney recipients. In summary, we have this 60 yo man interested on a seco..."
Renal Fellow Network: Doc, I am very sensitized!
Renal Fellow Network: Doc, I am very sensitized!: "Another day of transplant clinic… I heard from my attending that a couple is here for a second opinion about a kidney transplant. The husban..."
IN THE NEWS- Kidney biopsy Real Time Simulation
Using porcine and bovine and turkey breasts from local grocery stores and creating a simulation environment to teach nephrology fellows real time US guided kidney biopsy is described in this latest article from Kidney International.
have a look at this. This is very interesting inexpensive teaching tool
http://www.ncbi.nlm.nih.gov/pubmed/20631676
have a look at this. This is very interesting inexpensive teaching tool
http://www.ncbi.nlm.nih.gov/pubmed/20631676
TOPIC DISCUSSION: MINOXIDIL for Hypertension? what is the evidence?

Many nephrologists and internists use Minoxidil for resistant hypertension. What is the evidence of this medication in this current era of hypertensive management?
Minoxidil is a direct acting vasodilator. The usual dose is 5mg once a day and can be given as high as 100mg/day in divided dose. It was first used in early 19790s. Minoxidil's effect can be limited because of an increase in pulse rate and/or sodium (and water) retention. The latter may prove quite debilitating in some patients. Thus, minoxidil is generally administered with both a diuretic and an agent that can keep pulse rate in check, such as a ß blocker or a combined -ß blocker. The prominent tachycardia with minoxidil can aggravate myocardial ischemia and, if long-standing, leads to left ventricular hypertrophy. Minoxidil has a particularly annoying side effect of hypertrichosis that may limit its use, particularly among women. But someone with severe renal diseases, this drug can be quite effective.
In large measure, minoxidil acts by opening adenosine triphosphate-sensitive potassium channels in vascular smooth muscle cells. The major site of minoxidil action is arterial. Venodilation does not occur with minoxidil; thus, postural hypotension is unusual with its administration. The arterial vasodilatation leads to increased sympathetic activity. In conjunction with activation of the sympathetic system, both pulse rate and cardiac output increase with minoxidil; however, cardiac output and heart rate will tend to revert to pretreatment values with long-term treatment. And that’s the reason they get very tachycardic and should be on a beta blocker as well.
Another major problem is fluid retention. Why is that? The use of an arterial vasodilator will activate the renin system leading to ultimate activation of aldosterone and salt absorption. Hence it works well with Diuretic in place. Most patients who have been started on minoxidil are probably already on an ACEI, ARB and a diuretic and there is resistant hypertension.
Data on these drugs dates back to 1970s and very few studies. Look below for the references. No recent data exists on this medication. No data clearly for CKD patients.
But, even with this scant data, as a last resort, the drug is used frequently in patients with chronic kidney disease (CKD) who have been unresponsive to other antihypertensive medications. Most forms of hypertension, independent of severity and/or the degree of renal insufficiency, are at least partially responsive to minoxidil. In this regard, shortly after minoxidil was made available, it quickly replaced bilateral nephrectomies as the treatment of choice in advanced CKD patients with otherwise uncontrollable hypertension.
Minoxidil does not adversely affect renal function in the majority of patients with hypertension and a normal glomerular filtration rate (GFR). Basically, you get good control of their blood pressure and perhaps might even improve their GFR.
How many think that this medication works? And have used it a lot?
Any thoughts? Here are some old references. Not many articles recently on the use of this agent since 1980s. Only review articles recently
Any thoughts? Here are some old references. Not many articles recently on the use of this agent since 1980s. Only review articles recently
References:
Monday, September 20, 2010
Friday, September 17, 2010
Concept map of Types of Hypertension
Here is a VERY simplistic view of HTN:- Volume Mediated, Renin Mediated and Catecholamine Mediated.
Here is a concept map regarding that concept!

Here is a concept map regarding that concept!

Concept Map of Treatment of BK Nephritis

Here is a concept map of BK Nephritis Pathology and Treatment options
Thursday, September 16, 2010
JOURNAL CLUB: Early initiation of dialysis compared to national average
In the recently published IDEAL study, a comparison was made between early versus late initiation of dialysis. Among early start group, 18.6% started dialysis with an estimated GFR of less than 10 ml per minute. And in the late start group, 75.9% started dialysis with an estimated GFR of more than 7 ml per minute. At the time of dialysis initiation, the mean estimated GFR was 12ml per minute in early and 9.8 ml/min in the late start group.
During a median follow up period of 3.59 years, 152 of 404 patients (37.6%) in the early start group died, ie 10.2 events per 100 patient years. ( Mean age 60.2). If we compare this data with national data on ANZDATA:
http://www.anzdata.org.au/anzdata/AnzdataReport/32ndReport/AppendixI.pdf
Australia:
Year Deaths HD %age(Calculated)
2002 1048 7264 14.4
2003 1120 7722 14.5
2004 1208 8007 15.0
2005 1202 8637 13.9
2006 1326 9259 14.3
2007 1459 9701 15.0
2008 1482 10,062 14.7
NEW ZEALAND
Year Deaths HD %age(Calculated)
2002 232 1596 14.5
2003 264 1714 15.4
2004 306 1779 17.2
2005 298 1878 15.8
2006 333 1996 16.6
2007 296 2068 14.3
2008 356 2099 16.9
So as compared to national average, the mortality in the early start group, 10.2 per 100 patient years, appear to be significantly lower. The results are not statistically significant when compared to late start group, which might be because of significant overlap between the timing of initiation of HD, as discussed today.
Any thoughts !!!!!!!!!!
Reference:
http://www.ncbi.nlm.nih.gov/pubmed/20581422
During a median follow up period of 3.59 years, 152 of 404 patients (37.6%) in the early start group died, ie 10.2 events per 100 patient years. ( Mean age 60.2). If we compare this data with national data on ANZDATA:
http://www.anzdata.org.au/anzdata/AnzdataReport/32ndReport/AppendixI.pdf
Australia:
Year Deaths HD %age(Calculated)
2002 1048 7264 14.4
2003 1120 7722 14.5
2004 1208 8007 15.0
2005 1202 8637 13.9
2006 1326 9259 14.3
2007 1459 9701 15.0
2008 1482 10,062 14.7
NEW ZEALAND
Year Deaths HD %age(Calculated)
2002 232 1596 14.5
2003 264 1714 15.4
2004 306 1779 17.2
2005 298 1878 15.8
2006 333 1996 16.6
2007 296 2068 14.3
2008 356 2099 16.9
So as compared to national average, the mortality in the early start group, 10.2 per 100 patient years, appear to be significantly lower. The results are not statistically significant when compared to late start group, which might be because of significant overlap between the timing of initiation of HD, as discussed today.
Any thoughts !!!!!!!!!!
Reference:
http://www.ncbi.nlm.nih.gov/pubmed/20581422
Wednesday, September 15, 2010
IN THE NEWS- Basophils add fuel to LUPUS fire!

Recently, a nice basic science paper in Nature Medicine found some possible role of basophils in the pathogenesis of lupus. Using mice models, they showed that activation of basophils by autoreactive IgE causes the homing of lymph nodes promoting more TH2 cell differentiation and enhancing self reactive antibodies and leading to lupus like nephritis. Apparently humans with SLE have elevated serum IgE, self reactive IgE and activated basophils and can cause this second hit and worsening lupus nephritis.
In these experiments, B cell regulator was deficient and that led to spontaneous development of Anti DSDNA and lupus like nephritis and elevated IL-4 and IgE suggesting a role of Basophils, as they use the TH2 dependent pathway. So the postulated pathway is LUPUS disease has activated Ig E immune complexes and autoantigens and that activates basophils which upregulates MHC Class II and CD62L and IL-4 initiation that will eventually activate B cells and autoantibody formation leading to lupus nephritis!
A nice editorial in NEJM following this points out few important limitations. If the above was the case of pathogenesis of lupus nephritis, then almost all SLE patients should have IgE activation but only 30% of patients have detected auto antibodies to IgE. This talks only about a TH2 mediated pathogenesis but Th17 has also been implicated in lupus nephritis.
Few thoughts: Wonder how Rituximab affects basophils? If this is a possible mechanism, then every patient with Job Syndrome should get Lupus?
references:
http://www.ncbi.nlm.nih.gov/pubmed/20512127
http://www.ncbi.nlm.nih.gov/pubmed/20586122
http://www.ncbi.nlm.nih.gov/pubmed/20825323
Nephrology Crosswords

Just published in Kidney International
http://www.nature.com/ki/journal/v78/n7/abs/ki2010202a.html
Tuesday, September 14, 2010
Time to SINK with the WNK
I recently saw an interesting case of Familial Hyperkalemic Hypertension ( Gordon's Syndrome ) and read the current literature and role of WNK family of proteins. With-no-Lysine (K) kinases are family of proteins that have been found to play an important role in epithelial ions transport. They are involved in signaling in the sodium chloride and potassium transport in the aldosterone sensitive distal nephron. It is little bit complicated, but the figure will be easy to follow.
1.WNK4 inhibits NCC and ROMK
2.WNK1 stimulates ENaC and NCC through different mechanisms. Former through SGK-1 (Serum Glucocorticoid Kinase) and latter through inhibiting effect on WNK-4
3.Both WNK4 and WNK1 act synergistically to inhibit ROMK channel.
4.KS-WNK1 suppress NCC transport via its dominant negative effect on WNK1, stimulates ROMK activity via the same antagonistic mechanism and enhances ENaC-mediated transport through a different process
These observations suggest that, under certain physiologic circumstances, aldosterone simultaneouly downregulates electroneutral transport via NCC and enhances electrogenic transport via ENaC and ROMK
Gordon's syndrome is caused by mutations in WNK4 and WNK1 causing overactivity of NCC and inhibiting ROMK leading to hypertension and hyperkalemia. Other associated features are hypercalciuria and distal RTA, suggesting that atleast a subset of patients carry essentially a phenotype that is essentially a "mirror image" of Gietelman's Syndrome. The best way to remember these 2 syndromes is to be familiar with the features of thiazides.
CLINICAL CASE 25, ANSWERS and SUMMARY
A 87 y old patient comes in with ANCA negative Active RPGN, biopsy confirms pauci immune RPGN. Patient's presenting crt is 5.0mg/dl and quickly rises to require hemodialysis? What induction treatment would you choose?
Oral Cyclophosphamide + steroids + plasmapheresis 10%
IV Cyclophosphamide + steroids + plasmapheresis 68%
Steroids only 4%
Rituximab + steroids+ plasmapheresis 2%
Rituximab + steroids only 0%
Mycophenolate + steroids 2%
Do not treat as age is limiting factor 12%
Interesting break down. First and foremost. This is a tough situation. Although the age group where we see ANCA vasculitis is in the 65+ age group, as the age advances, the question always comes up- is the treatment more harmful than the disease?
I think that there were a fair number 12% that didn't want to treat. I think thats reasonable.
Now, the data on ANCA+ vasculitis is there but not that great. Usually most studies have used PO cytoxan and not IV cytoxan and recently two trials in the NEJM 2010 compared IV cytoxan in one trial to Rituximab and other PO cytoxan with rituximab. One can postulate that IV cytoxan would work as well. I think that both IV and PO cytoxan would be ideal answers along with Pheresis and steroids. I was surprised that not many of you chose rituximab given the latest findings. There is just observational data on MMF in this disease.
Now, all the data I have been talking about are in ANCA+ vasculitis. The case above was an ANCA negative pauci immune vasculitis. You can guess how much data is on that disease. Most of us would treat very similar to ANCA + vasculitis and possible remove any bad humor that is causing this vasculitis, perhaps its LAMP-2 antibodies some might say. Some might call it Atypical ANCA. 20-30% of microscopic polyangitis and Wegener's is ANCA negative. The treatment probably should remain the same, but the data is skimpy!
Here are some prior posts from us on this regard:
Sunday, September 12, 2010
Concept Map of FGF23 Pathology
Here is a concept Map I created of FGF23 pathophysiology with many disorders.
The article which has the most information I got from is listed below

References
http://www.ncbi.nlm.nih.gov/pubmed/20507943
The article which has the most information I got from is listed below

References
http://www.ncbi.nlm.nih.gov/pubmed/20507943
The Online Transplant Center
Please check out our sister site - The Online Transplant Center for latest updates and thoughts on transplantation medicine and fun quizzes as well.

Can BK Virus serum PCR be a good marker for Net immunosuppression?

In the field of transplantation, we are struggling to figure out is the patient on which end of the spectrum, too little immunosuppresion or too much immunosuppression. Markers for rejection have been studied extensively and based on Luminex DSA one can monitor early signs of impending antibody rejection. But many centers are also developing aggressive screening strategies for BK Nephritis. This entity is usually seen as early as 2 weeks post transplant to as late as 7 years post transplant but usually in the first year or so.
I think that A BK serum PCR might be a good marker for NET immunosuppression. Someone who has lupus and has been treated with Cytoxan, Cellcept, Rituxan and has failed kidneys recently and then gets a transplant for the kidney and gets inducted with more immunosuppression might be the highest risk for BK Nephritis much earlier on due to their NET immunosuppresion being the highest. No one can really measure NET immunsuppression. There is a test available called " Cylex" or ImmuKnow . This is the physiology behind it:
"Phytohemagglutinin (PHA) is a non‐specific mitogen which can be used to stimulate cell division in CD4 T‐ lymphocytes regardless of their antigenic specificity or memory status. Therefore, PHA is considered to be a “global” stimulator of the immune system. The production of intracellular ATP is one of the first steps in cellular activation following stimulation with mitogens such as PHA. ATP is a multifunctional nucleotide which plays an indispensible role in the transfer of intracellular chemical energy. The amount of ATP generated can tell us the amount of CD4 T cell activation and the overall immune status of the patient( over or under immunosuppressed). " -from the cylex website( summarized)
But a cell activation can occur in setting on an infection as well and a similar down stream effect on the kidney. Steady monitoring of infectious agents like BKV might be the BEST marker we have to date to tell us " Hey there is too much immunosuppression on board" !
But might not be as simple as that...
Lets see what future studies hold...
Cidofivir for BK Nephritis
At that time, most people will treat with IV Immunoglobulins and see if there is some response in terms of preventing rejection and treating BK at the same time.
So far, no drug has directly targeted BK except Cidofivir. Cidofovir is an antiviral agent that demonstrates in vitro activity against murine polyomavirus and has been proposed for treatment of BKVN in renal allograft recipients. The dose usually recommended is 0.25mg/kg IV every 2 weeks for 8 doses total. This is a low dose and can be used for someone in already some graft dysfunction as cidofivir itself can causing ATN like injury( same as tenofivir). This low-dose cidofovir may be tolerated, even among renal transplant recipients with significant renal dysfunction due to BKVN. Prospective, controlled trials are warranted to further define the optimal dose, toxicity and potential role of cidofovir in renal transplant recipients with BK virus nephropathy.
http://www.ncbi.nlm.nih.gov/pubmed/18380832
http://www.ncbi.nlm.nih.gov/pubmed/16499584
Saturday, September 11, 2010
Renal Fellow Network: Interventional nephrology in fellowship training
Renal Fellow Network: Interventional nephrology in fellowship training: "Interventional nephrology is quickly becoming a sought after 'subspecialty' of nephrology. However, many training programs do not offer a s..."
Thursday, September 9, 2010
Paired Chain Donation
A nice letter to the editor in NEJM this week Sept 2010 reflects on the Kidney Paired Donation program from San Antonio, Texas. KPD, which matches a living donor with a compatible recipient in a tag-team approach among potential donor–recipient pairs, can achieve compatible transplant combinations.
Based on this letter, if performed at a national level, it would potentially result in approximately 2000 additional live-donor transplantations annually and reduce the number of patients on the waiting list.
This is a growing trend and many transplant centers are reaching out to do this in many different ways. Some via a paired donation and some via a chain that is started by an altruistic donor.
Have a look at the NEJM editorial
http://www.nejm.org/doi/full/10.1056/NEJMc1004959
http://www.ncbi.nlm.nih.gov/pubmed/20061914
Based on this letter, if performed at a national level, it would potentially result in approximately 2000 additional live-donor transplantations annually and reduce the number of patients on the waiting list.
This is a growing trend and many transplant centers are reaching out to do this in many different ways. Some via a paired donation and some via a chain that is started by an altruistic donor.
Have a look at the NEJM editorial
http://www.nejm.org/doi/full/10.1056/NEJMc1004959
http://www.ncbi.nlm.nih.gov/pubmed/20061914
Wednesday, September 8, 2010
Topic Discussion: Renal Replacement Therapy in the ICU
A nice review in recent Nephrology Nature Review discusses the evidence of issues regarding Continuous Renal Replacement Therapy.
Few questions had arisen, few answered and few unanswered according to this review
1. What is the right CRRT dose? Based on the ATN and RENAL trial, both found that no specific mortality benefit was reached with high dosing of RRT. One should favor conventional dosing target of 20-25ml/kg/hr.
2. What is better CRRT or IHD in ICU patients? NOT evidence based but concensus is in favor of using CRRT in unstable patients who are critically ill
3. Timing of CRRT: When to start? early vs late vs never? Not compared or studied well
4. Do outcomes change: Few studies showed no mortality benefit. But article suggests the focus should be on Renal outcomes and not mortality? So not resolved yet
5. Which modality to use: CVVH vs CVVHD vs CVVHDF vs SCUF in the right setting. No real studies but all might be equivalent in the long run!
Check it out
http://www.ncbi.nlm.nih.gov/pubmed/20644583
Few questions had arisen, few answered and few unanswered according to this review
1. What is the right CRRT dose? Based on the ATN and RENAL trial, both found that no specific mortality benefit was reached with high dosing of RRT. One should favor conventional dosing target of 20-25ml/kg/hr.
2. What is better CRRT or IHD in ICU patients? NOT evidence based but concensus is in favor of using CRRT in unstable patients who are critically ill
3. Timing of CRRT: When to start? early vs late vs never? Not compared or studied well
4. Do outcomes change: Few studies showed no mortality benefit. But article suggests the focus should be on Renal outcomes and not mortality? So not resolved yet
5. Which modality to use: CVVH vs CVVHD vs CVVHDF vs SCUF in the right setting. No real studies but all might be equivalent in the long run!
Check it out
http://www.ncbi.nlm.nih.gov/pubmed/20644583
Tuesday, September 7, 2010
Quiz 5 Answers
Which one of the following is not a risk factor for PTLD
EBV status of donor/recipient 2 (16%)
Prior malignancy 1 (8%)
"Net" immunosuppresion 1 (8%)
Prior BK Virus infection 6 (50%)
Age 2 (16%)
Most of you got this one right away!
All except Prior BK infection has been associated to be a risk factor for PTLD In kidney transplant recipients
Please review the recent updated PTLD presentation by Arun Chawla for further clarification
http://onlinetransplantcenter.blogspot.com/search/label/presentations
EBV status of donor/recipient 2 (16%)
Prior malignancy 1 (8%)
"Net" immunosuppresion 1 (8%)
Prior BK Virus infection 6 (50%)
Age 2 (16%)
Most of you got this one right away!
All except Prior BK infection has been associated to be a risk factor for PTLD In kidney transplant recipients
Please review the recent updated PTLD presentation by Arun Chawla for further clarification
http://onlinetransplantcenter.blogspot.com/search/label/presentations
CONSULT ROUNDS: Adipsic Hypernatremia
THIRST mechanism is very important!

Tight regulation of water balance is accomplished via the thirst mechanism and antidiuretic hormone (AVP). Both are crucial to maintaining a remarkably narrow range of plasma osmolarity of 282-298 mOsm/kg. Osmoregulation of AVP is mediated by osmoreceptors located in the anteromedial hypothalamus near the neurohypophyseal cell bodies in the supraoptic nucleus. These osmoreceptors are extremely sensitive to changes in osmotic pressure. For example a decrease in osmolarity of 1-2% suppresses AVP secretion to permit maximum water diuresis. Non-osmotic variables such as reductions in blood volume or arterial pressure can also effect AVP secretion. Nausea is also well known to be a potent stimulus for AVP secretion.
However, AVP secretion alone is not adequate to prevent dehydration and an intact thirst mechanism is vital for water homeostasis. Thirst is regulated by hypothalamic osmoreceptors that are sensitive to changes in effective osmotic pressure of body fluids. The osmotic threshold at which thirst mechanism is activated begins approximately 5 to 10 mOsm higher than the threshold for AVP release. These two systems work together to maintain plasma osmolality. With both systems intact, development of hypernatremia mostly occurs in patients who have lost their ability to maintain or increase free water intake, for example hospitalized patients and particularly the geriatric population. A much rarer cause of hypernatremia from decreased intake are adipsic disorders, where an alteration in the thirst mechanism prevents patients from taking in adequate free water despite elevations in plasma osmolarity.
Defects in ADH synthesis or secretion cause central diabetes insipidus(CDI) or in some instances a partial CDI. These patients are polyuric and cannot concentrate their urine but maintain normal serum osmolarity with drinking large amounts of water. The thirst mechanism is intact. These patients do relatively well till they physical cannot drink water or their access to free water is lost. Conversely, a lesion in the thirst center in the hypothalamus can lead to an abnormal or no thirst response to hyperosmolarity but a normal ADH response. A defect in osmoregulated thirst mechanism is termed hypodipsic or adipsic hypernatremia . It is frequently associated with defective ADH production as well, either a CDI or partial DI. Due to lack of thirst sense, patients with this condition may fail to drink spontaneously and are at risk of hypernatremia. This risk is compounded by the fact that many of them also have an ADH production defect.
Disorders characterized by adipsia are uncommon, but a significantly large number of cases have been now described in the literature. There are four main patterns of abnormal osmoregulatory function. Type A adipsia is characterized by an upward setting of the osmotic threshold for both thirst and vasopressin release, sometimes called essential hypernatremia. Type B adipsia is characterized by subnormal thirst and vasopressin responses to osmotic stimuli. This is due to partial destruction of the osmoreceptors. Complete destruction of these receptors is classified as type C adipsia and these patients have complete absences of ADH release and a lack of thirst mechanism. Type D is an extremely rare form that manifests as only a thirst mechanism failure with an intact ADH production. Some might term these adipsic disorders as thirst regulation failures with a partial CDI or complete CDI.
However, AVP secretion alone is not adequate to prevent dehydration and an intact thirst mechanism is vital for water homeostasis. Thirst is regulated by hypothalamic osmoreceptors that are sensitive to changes in effective osmotic pressure of body fluids. The osmotic threshold at which thirst mechanism is activated begins approximately 5 to 10 mOsm higher than the threshold for AVP release. These two systems work together to maintain plasma osmolality. With both systems intact, development of hypernatremia mostly occurs in patients who have lost their ability to maintain or increase free water intake, for example hospitalized patients and particularly the geriatric population. A much rarer cause of hypernatremia from decreased intake are adipsic disorders, where an alteration in the thirst mechanism prevents patients from taking in adequate free water despite elevations in plasma osmolarity.
Defects in ADH synthesis or secretion cause central diabetes insipidus(CDI) or in some instances a partial CDI. These patients are polyuric and cannot concentrate their urine but maintain normal serum osmolarity with drinking large amounts of water. The thirst mechanism is intact. These patients do relatively well till they physical cannot drink water or their access to free water is lost. Conversely, a lesion in the thirst center in the hypothalamus can lead to an abnormal or no thirst response to hyperosmolarity but a normal ADH response. A defect in osmoregulated thirst mechanism is termed hypodipsic or adipsic hypernatremia . It is frequently associated with defective ADH production as well, either a CDI or partial DI. Due to lack of thirst sense, patients with this condition may fail to drink spontaneously and are at risk of hypernatremia. This risk is compounded by the fact that many of them also have an ADH production defect.
Disorders characterized by adipsia are uncommon, but a significantly large number of cases have been now described in the literature. There are four main patterns of abnormal osmoregulatory function. Type A adipsia is characterized by an upward setting of the osmotic threshold for both thirst and vasopressin release, sometimes called essential hypernatremia. Type B adipsia is characterized by subnormal thirst and vasopressin responses to osmotic stimuli. This is due to partial destruction of the osmoreceptors. Complete destruction of these receptors is classified as type C adipsia and these patients have complete absences of ADH release and a lack of thirst mechanism. Type D is an extremely rare form that manifests as only a thirst mechanism failure with an intact ADH production. Some might term these adipsic disorders as thirst regulation failures with a partial CDI or complete CDI.
A nice review is listed below in this topic
http://www.ncbi.nlm.nih.gov/pubmed/17371462
http://www.ncbi.nlm.nih.gov/pubmed/6727142
A talk on Urine Electrolytes part 2
Check out my talk on urine electrolytes
http://blog.ecu.edu/sites/nephrologyondemand/?p=4397
http://blog.ecu.edu/sites/nephrologyondemand/?p=4397
Monday, September 6, 2010
Post Kidney Transplant Renal Injury!
A Short Reminder!
We encounter acute renal failure always in the post transplant period
Besides the traditional pre renal, renal and post renal way of looking at the causes of renal injury post transplant, a mnemonic I learned from my mentors was : SCRI
or short for serum creatinine.
S- STRUCTURAL CAUSES
C- Calcineurin Toxicity
R- Rejection, any type/ Recurrence of primary disease
I- Infection, usually BK
The causes of proteinuria post transplant( major causes)
Rejection
Recurrence
De novo Glomerular Disease
Transplant Glomerulopathy
Post Transplant Collapsing FSGS
We encounter acute renal failure always in the post transplant period
Besides the traditional pre renal, renal and post renal way of looking at the causes of renal injury post transplant, a mnemonic I learned from my mentors was : SCRI
or short for serum creatinine.
S- STRUCTURAL CAUSES
C- Calcineurin Toxicity
R- Rejection, any type/ Recurrence of primary disease
I- Infection, usually BK
The causes of proteinuria post transplant( major causes)
Rejection
Recurrence
De novo Glomerular Disease
Transplant Glomerulopathy
Post Transplant Collapsing FSGS
Sunday, September 5, 2010
TOPIC DISCUSSION: Brief Concept Map of Hypercalcemia Causes
Here is an image of overall big picture causes of Hypercalcemia that I could come up with in a concept map format. A picture of the this is worth a 200 word blog.


CONSULT ROUNDS: CAUSES OF UPJ OBSTRUCTION
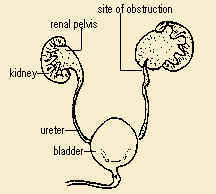
The most common causes are usually
Congenital
Strictures
Crossing vessel or band pressing on the UPJ
Instrinsic Stenosis
Decreased peristalsis through UPJ
Other less common causes
Renal Cyst at that location
Aortic Aneurysm
Eisonophilic ureteritis
Xanthogranalumatous Pyelonephritis
What do they mean by crossing vessel?
In adults, the obstruction of the ureter can be caused by an extra blood vessel, usually an artery that supplies the lower part of the kidney. As a person gets older, this vessel gets bigger. Since this blood vessel will usually lie over the ureter, it can cause obstruction. This is called a "crossing vessel".
http://www.ncbi.nlm.nih.gov/pubmed/19193425
Wednesday, September 1, 2010
Subscribe to:
Comments (Atom)